
(Around 63 children have died in the last five days in Gorakhpur (UP) district’s BRD Medical Hospital. Reports allege that the probable causes of deaths were low supply of oxygen and in some cases, encephalitis syndrome. The Quint is republishing this article from 26 August 2016 on the deadly Japanese encephalitis and why it requires the government’s immediate attention.)
Panic gripped Manipur in July 2016, when a four-year-old girl – after suffering high fever, convulsions, and slipping in and out of consciousness over a few days –succumbed to Japanese encephalitis (JE), the state’s first death from the viral brain infection transmitted by the Culex mosquito since 2010. A few days later, the virus claimed its second victim, an adult.
These deaths were enough to close schools until the end of July in the district of Churachandpur and spark a reaction in the parliament a fortnight ago, as MPs asked what India had to show despite years of efforts to contain JE, caused by a virus that is a cousin of those that cause dengue and yellow fever, all impervious to medicine.
This is why JE requires more government attention than it presently gets:
- JE is the leading cause of viral encephalitis or brain inflammation in Asia. While mild cases of JE experience fever with headache, much like any other viral fever, severe infections are associated with neck stiffness, stupor, disorientation, coma, tremors, convulsions and spastic paralysis. Fatality rates for severe infections hover between 20 percent and 30 percent, according to the World Health Organization (WHO).
- Even with treatment, JE can leave significant neurological effects, especially in children. About 30 percent to 50 percent of the survivors can struggle to walk or suffer cognitive disabilities. With poliomyelitis nearly eradicated, JE is now the leading cause of childhood viral neurological infection and disability in Asia.
- JE is caused by a virulent virus. Much like Manipur this year, the virus made a comeback in Odisha in 2012, after two decades, with 272 cases reported and 24 dead.
- JE has a tendency to invade new areas that host its traditional habitat—stagnant water in paddy fields—and even develop in new habitats. “Sub-groups of the Culex species of mosquito have been found in vegetation growth along the Yamuna, from where they are infecting people,” said AC Dhariwal, director, National Vector Borne Disease Control Programme (NVBDCP).
India’s JE Burden Much Higher Than Reported
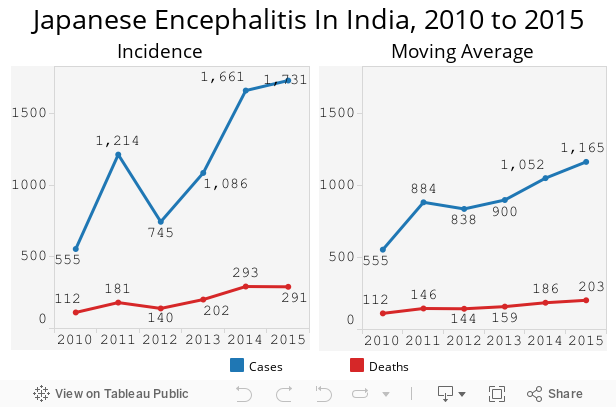
In March 2016, IndiaSpend reported a 3 percent decline in allocations to the National Vector-Borne Disease Control Programme, which covers malaria, dengue, chikunguniya and JE, kala-azar and lymphatic filariasis, from Rs 482 crore in 2011-12 to Rs 463 crore in 2015-16.
Over this time, JE – thus named because it was first reported in Japan in 1871–cases rose by 210 percent while the death toll rose by 181 percent.
JE cases could be many times the officially reported data, according to this 2016 study in the Journal of Paediatrics, because the testing method popularly used to detect the virus infection in the patient’s blood and cerebrospinal fluid may be missing cases of JE among patients of acute encephalitis syndrome, a brain fever.
We estimated 626 symptomatic JE cases in Kushinagar, a district in Uttar Pradesh (UP), in 2012, while the state of UP reported 139 confirmed cases during the same transmission season.Manish Kakkar, Associate Professor with the Public Health Foundation of India (PHFI).
The global burden of JE could be 10 times the figures reported to the WHO, a 2011 study estimated.
Adults as Susceptible to JE as Children
Traditionally, children were the most affected age-group by JE, said the NVBDCP’s director, Dhariwal. Infection rates in children aged three to 15 were found to be 5 to 10 times higher than in adults, according to this 2012 study.
Since vaccination offers significant protection against JE, in 2006, the government launched immunisation campaigns for children aged one to 15 in UP’s endemic areas—regions where infection rates are maintained in a population without the need for external inputs.
Campaigns are the first line of action against JE, the second being routine immunisation, after covering the vulnerable population group through campaigns.Pradeep Haldar, Deputy Commissioner at the health ministry
The NVBDCP has declared 216 districts endemic for campaigns, 17 in the current transmission season alone.
Immunisation against JE is part of routine immunisation (RI) in 197 districts. Two doses are administered, the first at about nine months, the second at 18 months.
Good immunisation coverage has helped curtail the outbreaks of JE in south India like in Tamil Nadu, Andhra Pradesh, Karnataka, and some districts of UP, Bihar, etc.AC Dhariwal
However, as we said, JE finds new targets. With children better protected, the virus is striking more adults. This 2015 study of 778 patients in Assam found adults more vulnerable, possibly due to exposure in paddy fields. Manipur alone recorded 19 adults and 12 children with JE in the ongoing season, according to the state’s surveillance office. This raises the question of adult vaccination.
So far, adult vaccination campaigns have been implemented in 21 “high-burden districts” identified by the NVBDCP in Assam, West Bengal and Uttar Pradesh, with another 10 districts about to be declared endemic, said Haldar.
There is no shortage of funds for immunisation.Pradeep Haldar
Districts are declared endemic and receive vaccination-priority based on evidence. But ground reports suggest people demand quicker, faster action.
In Manipur, public awareness about the protective benefit of vaccination is high, said Thokchom Nandakishwor Singh, State Nodal Officer (Immunisation), Manipur. So, a vaccination drive in July for those under 16 was conducted with police support to manage the crowd that turned up, with adults clamouring to be vaccinated.
Nandakishwor advocates adult immunisation in highly susceptible areas, “but this is not under my jurisdiction”, he said.
Apathy, Rickety Rural Healthcare Increase Deaths
No medicine exists to treat JE. As with other viruses, patients are treated for the symptoms they develop.
Serious cases can be prevented from developing complications by the early management at the primary and secondary level.
...but this pattern is often not followed in rural areas where outbreaks happen.Kakkar
For instance, in districts in eastern UP’s Gorakhpur division, classified “high endemic”, the chances of death increase because people cannot afford transfers to better health centres.
The apathy of government doctors to register deaths as attributable to JE, and hence frequent referrals to shift serious patients out of their care, further increase the chances of patients succumbing.Manish Kakkar
The lack of attention in remote areas spurs an influx of “serious” patients in urban hospitals sufficiently equipped to handle critical cases. This year, so far, five JE cases—four adults, three male, one female, and one 12-year-old boy—from smaller towns have sought treatment at the Shija Hospitals & Research Institute, one of Imphal’s best private hospitals. Three of those cases needed ventilator support.
It’s been the worst year for JE in recent times, the virus becoming more virulent.Chetan Khundongbam, residential medical officer at Shija
At the time of this interview, four of five cases had been discharged after full recovery. Khundongbam was treating a 58-year-old man, brought in from a remote region with high fever, neck rigidity, drowsiness and convulsions. He was critical and on ventilator support.
Change in Cropping Pattern Expose Population to JE
When JE was detected in India, in 1955 – 84 years after the first case in Japan – the disease was confined to Tamil Nadu. In 1973, it struck West Bengal. The virus then invaded 22 rice-growing states, where its carrier, the Culex mosquito, breeds in stagnant water, acquiring the infection from feeding on infected domestic pigs, the amplifying host, and migratory birds, the natural host.
Uttar Pradesh first reported JE in 1977. However, outbreaks in Gorakhpur and neighboring districts have become more frequent and intense after the late 1970s, when more farmers switched from sugarcane cultivation to paddy, said the NVBDCP’s Dhariwal.
In Haryana, the latest region to suffer JE outbreaks, the Culex mosquito has found a new habitat–vegetation along the Yamuna.
Back in the Northeast, Assamese doctors have blamed warmer temperatures for an extended transmission season, lasting up to November instead of July, and for the rising number of cases in the state.
(Published in arrangement with IndiaSpend.)